Historians often demure when asked what concrete lessons can be drawn from the past. Meanwhile, purported irrelevance threatens the place of the humanities in higher education. That crisis of confidence, made more urgent by the COVID-19 pandemic, calls for a renewed engagement with practical questions and public audiences. What lessons can be drawn from the interrelated histories of disease, environment, and medicine? This roundtable invites four scholars of Middle East history to reflect on a series of questions to illuminate the current moment–in the region and beyond–with their research.
The roundtable consists of me, Joelle Abi-Rached (Columbia), A. Tylor Brand (Trinity College, Dublin), and Seçil Yılmaz (Franklin and Marshall). Definitely worth checking out if you’re interested in the history of medicine and how it plays into environmental history.
Proving that I can write about things other than the Spanish flu …
In the summer and fall of 1883, the newly-installed Anglo-Egyptian government faced its first public health crisis when cases of cholera were reported in the Nile Delta and rapidly spread throughout the country. The government’s response was based in part on long-standing European prejudices about the “Orient” as the origin of plague and pestilence and “Orientals” as people who did not understand health, science, or hygiene, and were unconcerned—even fatalistic—in the face of life-threatening illnesses.
To the contrary, Egypt had, over the course of the 19th century, developed a basic national health system, which had earned praise from European observers prior to the British occupation in 1882. The prejudices expressed by British occupation authorities also elides the British government’s own stance in ongoing debates among European scientists about contagion and the appropriate methods for preventing the spread of diseases like cholera.
The Anglo-Egyptian government’s response was based on imperial policies, racial prejudices, and scientific understandings that failed to adequately deal with the pandemic at the cost of 50,000 Egyptian lives.
I wasn’t quite expecting 5,000 people to have an interest in the ‘Spanish’ flu in Egypt, but … well, 5,000 people have read my previous post, which was also translated into Arabic (not by me, fortunately). And then I was cited by both The New York Timesand Masry Al-Yawm, and have met (virtually) a few other people interested in the subject.
It’s been kind of exciting doing this all from the comfort and confines of my home, where I’m quarantined with a chemical engineer and three hyperactive cats (and a fourth who’s just above it all).
I’ve been trying to figure out what brilliant thoughts I could possibly use to follow up on the previous post, but none are immediately forthcoming, and they’re standing in the way of announcing, for those who are interested, this:
On Wednesday, May 6, 2020, at 3 PM U.S. Eastern time (8 PM London / 9 PM Cairo), I will be giving a lecture on “The Spanish Influenza in Egypt” for Harvard’s Islamic Studies program online. The talk will cover much of the material that’s in my forthcoming article–the one that won’t be out until next year–so, if you’re interested, you might want to tune in. (I don’t know if it will be archived).
I’m extremely honored to have been asked — the director of the program actually found me through my blog post! — and even more elated to follow the incomparable and brilliant Nükhet Varlık (Rutgers& U South Carolina), who is speaking on April 30th (also 3 PM Eastern) on “Rethinking the Plague in the Time of Coronavirus.” (You can RSVP for her talk at https://islamicstudies.harvard.edu/plague.)
I haven’t said much lately because I don’t have much to contribute to the ongoing panic/dialog around the COVID-19 pandemic. Since there’s so much noise out there, I’ve decided to adopt–well, on this website anyway–a less is more approach.
Within the last week or so, however, as the pandemic has settled in to different contexts worldwide, I’ve found myself recounting the story of the “Spanish flu” pandemic in Egypt. This has partly been because there has been some criticism of the way the current Egyptian government has handled the pandemic, and this has caused some questions about how, previously, such things have been handled in Egypt.
I’ve written an article on it that’s been accepted by the Journal of World History, but it likely won’t appear until 2021. I do have permission to share the article here and on my academia.edu profile once it’s out, but I feel like there’s a limit to how much of my own research I can discuss in public before it appears. (note: the key word here is in public. I can certainly respond to, say, questions that are posed, either below or by e-mail … )
However, the article is ten thousand words long, and a short blog piece about the pandemic in Egypt that addresses the questions I feel like I’ve been asked several times won’t venture too far into spoiler territory!
“Al-Anfilwinza al-Wafida.” Al-Muqattam, December 7, 1918, 2.
What was the “Spanish flu”?
So, first off, let’s all remember that it was called the Spanish flu because Spain’s uncensored press was the first to report on the unusual nature of the virus in the spring of 1918. It didn’t originate in Spain nor, as someone tried to argue with me on Twitter a few weeks ago, did it attract the name because more people died of it in Spain than anywhere else.
The pandemic lasted globally until 1920, and it went around the world in three waves. The second was the most lethal, although all three waves carried the same unusual mortality curve: in addition to the young and elderly, the highest mortality rates were observed in people aged 15-25.
The virus, a mutated strain of the H1N1 avian influenza, frequently caused victims to cough or spit up blood, their faces to turn purple or black, and, in victims with particularly robust immune systems, it caused their lungs to fill up with fluid. This latter was a frequent cause of death–misidentified as pneumonia early on–because the immune system was triggered into an over-response; fluid was produced in an attempt to counter the virus, and victims essentially drowned.
When did the pandemic hit Egypt?
The first wave of the pandemic appeared in Egypt sometime in late spring–around May or June. It attracted little attention, other than commentary on its appearance at an unusual time of year, and the Department of Public Health (a subset of the Ministry of the Interior) recommended that people should stay home if sick.
It wasn’t until the end of October–right around the time that the Treaty of Mudros was signed, ending Ottoman participation in World War I–that the lethal wave hit. The most lethal period of the pandemic persisted until just after Christmas, resulting in a large number of casualties in the last eight weeks of 1918.
The third wave is mentioned very briefly in the press–right after Sa’ad Zaghlul’s arrest in March 1919. Vital statistics–such as they are–seem to indicate that it was fairly mild, but given the fact that the country exploded into open rebellion and most government ministries were effectively shut down until midyear, it’s impossible to know for sure.
How did the Egyptian government deal with the pandemic?
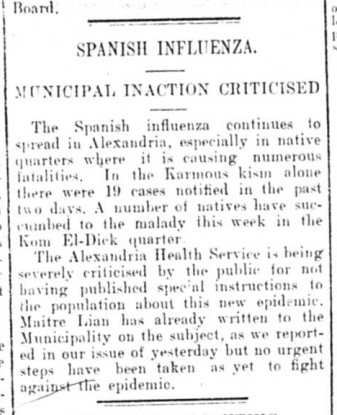
Egyptian Gazette, November 18, 1918
At the time, Egypt was a British protectorate. The system known as the “Veiled Protectorate,” wherein Egypt was administered by the British but there was lip service given to an official fiction that it remained an autonomous Ottoman province had been done away with upon the mutual declaration of war between Britain and the Ottoman Empire in November 1914. Egypt was declared a British protectorate–it would remain so until 1923–and placed under martial law at the beginning of December 1914 (this was cancelled as a gesture of goodwill by General Allenby in May 1919).
The problem in Egypt, as in other colonial settings, is that colonial officials who held military rank were recalled to duty for the war, and many of them had been sent into Palestine with Allenby’s campaign starting in the fall of 1917, and remained there at the time the pandemic’s most lethal wave arrived a year later. This included much of the leadership of the Department of Public Health as well as most of the district medical officials whose job was to oversee health services for the civilian population.
Simply put, for most of the war, civilian medical needs were a far distant second behind military medical needs (and for this, I’ll refer you to my book that’ll be out sometime in the next decade).
Hence, when the pandemic hit Egypt, the Anglo-Egyptian government was caught with its pants down. Hospitals and clinics were overwhelmed. A meeting of the Alexandria municipality in early November turned into an ad hoc grievance session, with citizens angrily demanding that the head of the Municipal Health Department do more to control the pandemic.
It was mid-November before basic guidelines were issued to the public; schools remained open until early December. Markets, courts, and universities were closed. Cities and provincial governments issued directives, but many seemed haphazard in their approaches: in Cairo, cinemas were closed, but not theaters; bars were closed, but not cafes. In both Cairo and Alexandria, people complained about crowding on the city’s tramways, with local governments feebly admitting they could do little to control the environment.
Physicians–who were mostly Egyptians, Greek, or Syrian–were overworked; at one point the press observed that in Asyut doctors were making constant housecalls and working over 15 hours a day. The next week it was reported that all of the city’s doctors had caught the flu themselves and were unable to see patients.
It was reported that in some rural villages there was “no other business other than to bury the dead,” and that agricultural production had ceased. This is extremely important to note, as the entire economy depended on intensive agricultural production, and most peasants had little savings. Stopping work in the fields would only have happened under the most extreme of circumstances.
Were religious services suspended in 1918 like they are now?
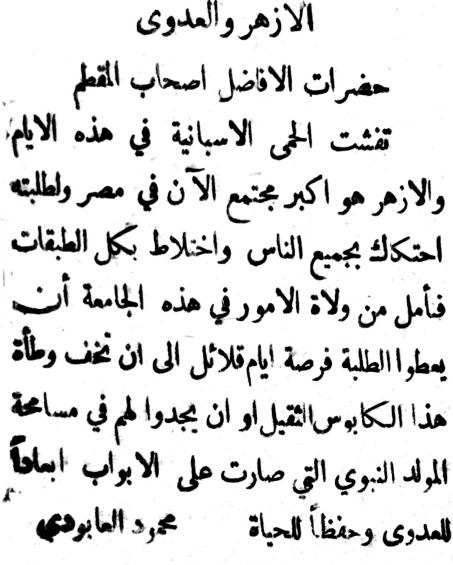
Al-Muqattam, December 3, 1918.
Update: if they were, it happened late. Al-Muqattam reported on December 6 (the height of the second, and most lethal wave) that the Alexandria Municipality’s Sanitary Department had asked the Ministry of Awqaf to make sure mosques were properly ventilated during prayer services, and that the floors were being cleaned with purified water before and after.
This question has come up several times, especially with Ramadan looming now (Ramadan didn’t coincide with the worst of the pandemic in 1918). The issue is suspicious by its absence from the press, in fact, but I don’t know what to make of it (if anyone knows, please leave a comment or message me!).
The Anglo-Egyptian administration was very wary of stepping on toes that should have been handled by the Ministry of Religious Affairs (most colonial administrators had experience working in India, where the 1857 revolt loomed large in memory, and the British tried not to offend Islamic sensibilities). Hence, when Al-Azhar was ordered to close–which it was–this was ordered in its capacity as an educational institution, not as a place of worship.
Public celebrations of Mawlid an-Nabi, the Prophet’s birthday, were cancelled, as were permits for religious processions as well as funeral processions. I have not seen references to mass graves (this had caused uproar during previous pandemics), but people were encouraged to conduct quiet burials as quickly as possible.
How many people died?
Egypt. Ministry of the Interior. Department of Public Health. Annual Report for 1918. Cairo: Government Press, 1920, 36.
The officially calculated death toll was 138,000 people — over 1% of Egypt’s population according to the census conducted in 1917.
That said, Niall P.A.S. Johnson and Juergen Mueller[1] wrote an article in 2002 to try to compile a more accurate global total of the pandemic’s mortality, and they concluded that the method used in Egypt as elsewhere usually produced estimates that were too low, sometimes by as much as half. Hence, it seems more likely that the death toll would be closer to 170,000; the overwhelming majority of these deaths taking place in the last eight weeks of 1918. (To clarify: Johnson and Mueller have said that the method was inaccurate; the estimate of 170,000 is mine.)
The highest mortality rate in Egypt was observed in people between the ages of 10 and 20, with rural areas more heavily affected than urban areas. (I do have a theory about why this is, but you’ll have to read the article).
To put it in context, this would be the generation of young men and women who were left behind to run farms and keep things going while fathers and older brothers went off to work in the Egyptian Labour Corps, the Egyptian Camel Corps, and other work associated with the war effort, as agricultural wages had remained relatively flat even as inflation sent the cost of basic goods upwards by as much as 300%. They would have gotten through the war, and then perished just as it looked like things might return to normal. Socially, this must have been devastating.
I do think this is one of the reasons why rural residents were angry and ready to express that anger when the 1919 uprising began. (In my book, which I am still working on, I argue that people were hungry for most of the war. The influenza–the worst health crisis during World War I in Egypt–came after the end of the war, and made everything worse.) Political organizers from the Wafd and other parties who went into rural areas probably had their work cut out for them.
The influenza has, oddly, been omitted or ignored in most of the histories of early 20th century Egypt. I’m hoping my forthcoming article can start a conversation about some of the non-political events in early 20th century Egypt that have long been set aside in favor of the political narrative that tends to be emphasized in scholarship of the period.
Talk to me!
Even though I’ve got an article coming out, I’m interested in comparing notes with anyone else who’s working on this or similar topics, just because there isn’t much out there. I’m especially interested in hearing family lore–did someone in your family tell stories about the pandemic? Or can you fill in some holes in the narrative? Leave a comment, or e-mail me!
Postscript
I wasn’t expecting this post to be so popular! I’m sorry that it’s not longer. I really wanted to just answer some of the usual questions, but I’m glad so many people are interested in the topic.
The Lecture I gave for Harvard on May 6, 2020 is now online:
A number of people on Twitter have said that they wished I’d written more about the political effect of the pandemic. I’m afraid that I just don’t have enough solid data to make stronger claims at this point.
I am still working on this, so if you have ideas please let me know.
1. Johnson, Niall P. A. S., and Juergen Mueller. “Updating the Accounts: Global Mortality of the 1918-1920 ‘Spanish’ Influenza Pandemic.” Bulletin of the History of Medicine 76, no. 1 (2002): 105–15. https://doi.org/10.1353/bhm.2002.0022.
Last week, I called a sitting United States Senator a dumbass on Twitter.
The viral (pardon the pun) response to the tweet was an exhilarating ride. I learned there’s a lot of people out there that just don’t like China. Many people decided to share a National Geographic article about a new theory that the pandemic originated in China, apparently having missed the part where the point of my tweet was that the virus didn’t originate in Spain, and misinterpreting what I meant when I said it was first detected in Kansas.
(There are also two other prevailing theories about its origin, none of which can be definitively proven, nor are universally accepted).
Many people accused me of having an agenda to hide the origin of the coronavirus outbreak (which I never mentioned). Some lobbed completely false information at me (when I said first detected, I meant globally, not in the US, but thanks for playing, “America’s best CPA”! And no, it was not called the Spanish flu because more Spaniards died than anyone else, you’re citing an undergraduate research project posted online in 1997.)
And, predictably, a lot of people just resorted to insults. After a professional troll broke my demeanor at the end of the day, I muted the conversation and, when the number of likes had doubled by the following morning, I made my account private for a couple of days.
So, how do diseases get their names, and what’s the issue with calling COVID-19 the “Chinese virus” anyway?
Diseases were frequently named for their symptoms: “choleric,” for example, was used to describe someone who became so angry their face turned deep red (a symptom of the disease that took the name “cholera”).
“Bubonic plague” was named because it caused “buboes,” or masses of swollen tissues in the armpits or groins of its victims.
“Whooping cough” because of the sound patients made.
Others–pneumonia, bronchitis–were named for the parts of the body chiefly afflicted.
When Europeans began trading with and traveling to regions outside of Europe, the diseases they encountered became a concern; this became doubly so with the expansion of settler colonialism in the 18th century.
Check out, for example, the title of James Lind’s 1768 treatise, An Essay on Diseases Incidental to Europeans in Hot Climates, with the Method of Preventing their Fatal Consequences.[1] Lind’s essay suggested that the stresses that European bodies encountered in regions of ‘hot climate’–writing about the West Indies, he mentions the temperature, humidity, and local ecology–made them more vulnerable to disease.
James Johnson, writing in 1821, offered a similar analysis in The Influence of Tropical Climates on European Constitutions, which was about the experience of Europeans in India.[2]
Through this developed an entire field of medicine, commonly called “Tropical Medicine,” born of the idea that European bodies could not dwell in tropical environments without medical intervention.
In the beginning, the possibility that native medical practitioners might have effective treatments for local diseases was considered, mostly in India where Europeans—French, Portuguese, and English among them—frequently sought medical assistance from hakims and vaidyas, “encouraged by a belief that local doctors would be more familiar with the diseases of the climate and with the locally occurring medicines an obliging nature had provided for their treatment.”[3]
Such measures were relatively common as late as the 19th century, but were ultimately discouraged by colonial administrators who preferred European methods to native, buoyed by the notion of science-as-progress. Admitting that the colonies could compete with the metropole in scientific output ran counter to the notion of the mission civilizatrice.
New institutions were set up, first in Liverpool and then in London, to train doctors in the new field of Tropical Medicine.
The London School of Hygiene and Tropical Medicine. I have a very complicated relationship with this place. (author photo, 2016).
As new diseases in the “tropics” were identified, they were frequently named for the regions where they were found, almost as a warning. Go here, and you will contract this disease. Abandon all hope.
The unfairness of German measles
Several people in my mentions last week brought up that old childhood malady in the United States: the German measles. It’s one of the archetypes of a misnamed disease, because it was identified as a separate strain by three German physicians at the beginning of the 19th century, and was so named “German.”
Aha, my critics said. Can’t explain that, can you?
I remain unclear what this was supposed to prove, since even simple playground logic posits that two wrongs don’t make a right.
But, ask yourself … when was the last time you heard the term “German measles”? It’s now commonly called rubella, and has been for quite some time. Why?
Well, you see, the name “German measles” was discouraged among medical professionals in order to avoid giving the impression that the disease was endemic to Germany, that Germans were predisposed toward it, or that Germans carried the disease and could transmit it to others.
Funny, that.
In which it gets racial
Several other people brought up Zika, Ebola, Middle East Respiratory Syndrome, and Southeast Asian Respiratory Syndrome — all problematic names as well. (I do, candidly, wonder how many people realize Zika and Ebola are places in Africa). Several people pointedly asked if the West Nile River had its feelings hurt by the disease named after it. (For the record, it was named for the West Nile region in Uganda, in 1937.)
One critic–who’s not wrong, by the way–lamented that there’s been very little attention paid to the diseases that come out of Africa and the names they bear.
Unfortunately, that problem is bigger than myself. But, yes, the names of all of these diseases suggest that these places where white people don’t live are inherently dangerous.
But, before I move on, let me touch one last time on the name “Spanish” influenza. The virus may have come from Kansas, France, China, or somewhere else, but we can be pretty certain it didn’t originate in Spain. And one commenter suggested that people are trying to clear Spain’s reputation because Spain is “white.”
Not so fast. This is also an oversimplification. Spain–and the Spanish–may be considered white now, but at the beginning of the 20th century this wasn’t necessarily the case, especially in the United States.
The US had fought a war with Spain, and they were our bogeyman. Other European powers weren’t huge fans either–Spain, along with the Ottoman Empire, was a Mediterranean imperial remnant, one that peaked around 1600 and was limping along in decadence (from the verb “to decay”), refusing to join the modern world.
At the time, the US was also engaged in an internal debate about whether to admit southern Europeans–non-Protestants, mostly poorer–as immigrants.
The Spanish, Italians, and Greeks may not have been considered “of color” but they weren’t considered equal to the “superior European races” like Britons, French, Germans, or Scandinavians.
Did this play into the popularity of the name “Spanish flu?” Almost certainly.
Coronavirus and COVID-19
Which brings us to coronavirus.
How many times have you seen someone reference “bat soup” in relation to the origin of the outbreak?
We don’t know who patient zero was, or how they contracted the virus. Yes, they probably lived in Wuhan (or in Hubei province).
And, yes, the coronavirus was detected a few years ago in bats. Most humans who contract illnesses from bats are bitten or handle diseased animals.
Have you once seen it suggested that, say, a sanitation worker who found a near-dead animal might have been patient zero?
Have you seen it suggested that someone out camping or hiking for the weekend was bitten by an infected animal?
No. Of course you haven’t.
You’ve seen references to people eating bat soup, because a media outlet went to Wuhan, and, without any actual evidence, found a local market serving bat meat and identified it as the place where the disease came from.
Let’s set aside the fact that properly cooked meat doesn’t transmit disease.
The reference to “bat soup” is intended to reinforce the foreign-ness and other-ness of China. The virus came from there. It is theirs. It comes from their weirdness.
We have a long history of doing this in the West: presenting China, specifically, as the antithesis of all that is Western–disease ridden humans at their most primal (well, except for Africa, whose humanity we’re barely likely to even acknowledge).
The question of blame
Did the Chinese government bungle its response to the coronavirus outbreak? You betcha.
So did the UK government, the American government, and a host of others.
In 2015, the World Health Organization issued guidelines on the naming of diseases that recommended against the inclusion of geographic names in order to prevent the stigma of association for residents of the area.
So, when politicians insist on calling the virus “Chinese,” what are they hoping to accomplish?
When the American president crosses out “coronavirus” on his prepared remarks and writes “Chinese virus” in magic marker in letters so large they can be seen off-podium, what is he hoping to accomplish?
When the Secretary of State sinks a joint G-7 statement on the virus over the insistence that it be called “Wuhan virus,” what is he hoping to accomplish?
Whenever I pose this question, I keep seeing “China needs to take responsibility” as an answer.
If China needs to be held accountable, sue the Chinese government for reparations and damages.
Everyone knows the virus came from China. I, myself, have never denied this.
But my question stands: what is us calling it “Chinese” to each other supposed to accomplish?
[1] James Lind, An Essay on Diseases Incidental to Europeans in Hot Climates. With the Method of Preventing Their Fatal Consequences. (London: Printed for T. Becket and P. A. de Hondt, in the Strand, 1768).
[2] James Johnson, The Influence of Tropical Climates on European Constitutions : Being a Treatise on the Principal Diseases Incidental to Europeans in the East and West Indies, Mediterranean, and Coast of Africa (United States, 1824), http://catalog.hathitrust.org/Record/008886165.
[3] Arnold, Colonizing the Body, 11; M. N. Pearson, “First Contacts Between Indian and European Medical Systems: Goa in the Sixteenth Century,” in Warm Climates and Western Medicine: The Emergence of Tropical Medicine, 1500-1900, ed. David Arnold, The Wellcome Institute Series in the History of Medicine, Clio Medica 35 (Amsterdam and Atlanta: Rodopi, 1996).